In a previous blog post, I summarized the new functional G-codes and what we can expect in 2013. This article will summarize how they work, how you report the measures and what is critical to remember.
CMS has defined categories of functional limitation that address “activity limitations” and “participation restrictions.” They have assigned specific G-Codes for each category. The categories for 2013 are:
- Mobility: Walking & Moving Around
- Changing and Maintaining Body Position
- Carrying, Moving and Handling Objects
- Self Care
- Other PT/OT Primary Functional Limitation
- Other PT/OT Subsequent Functional Limitation
- Swallowing
- Motor Speech
- Spoken Language Comprehension
- Spoken Language Expression
- Attention
- Memory
- Other SLP Functional Limitation
As you can see, by including “Other” Categories and a “Subsequent” category, CMS expects reporting to be comprehensive. They also expect it to be limited to only the primary limitation, but if that goal is met and treatment continues, CMS expects a subsequent limitation to be reported.
Each category has 3 related G-Codes: One to report current status, one to report projected goal status, and one to report discharge status. As an example, this is the Mobility code set:
| Mobility: Walking & Moving Around | |
| G8978 | Mobility: walking & moving around functional limitation, current status, at therapy episode outset and at reporting intervals |
| G8979 | Mobility: walking & moving around functional limitation, projected goal status, at therapy episode outset, at reporting intervals, and at discharge or to end reporting |
| G8980 | Mobility: walking & moving around functional limitation, discharge status, at discharge from therapy or to end reporting |
| Modifier Impairment Limitation Restriction | |
| CH | 0 percent impaired, limited or restricted |
| CI | At least 1 percent but less than 20 percent impaired, limited or restricted |
| CJ | At least 20 percent but less than 40 percent impaired, limited or restricted |
| CK | At least 40 percent but less than 60 percent impaired, limited or restricted |
| CL | At least 60 percent but less than 80 percent impaired, limited or restricted |
| CM | At least 80 percent but less than 100 percent impaired, limited or restricted |
| CN | 100 percent impaired, limited or restricted |
When reporting a functional limitation, the therapist is expected to assess and report the severity of the limitation as well. This will be done through the use of seven (7) modifiers.
Therapists determine severity by using a valid and reliable measure or assessment tool. Therapists can use more than one tool and use their professional judgment when selecting the appropriate modifier. It has been well-commented that converting non-linear measures to a percent scale doesn’t translate well to functional improvement, and that is why there is specific language around using professional judgment in assessment. But, it must be supported in your documentation.
How do you report the measures?
CMS has provided a rather ugly chart that demonstrates when each code is required for submission. The take away is when you start treatment, submit your initial finding and your goal. At least every 10 treatment days submit your current finding and your goal. At discharge submit the goal and the final finding. If you complete one goal and add a subsequent goal, just rinse and repeat.
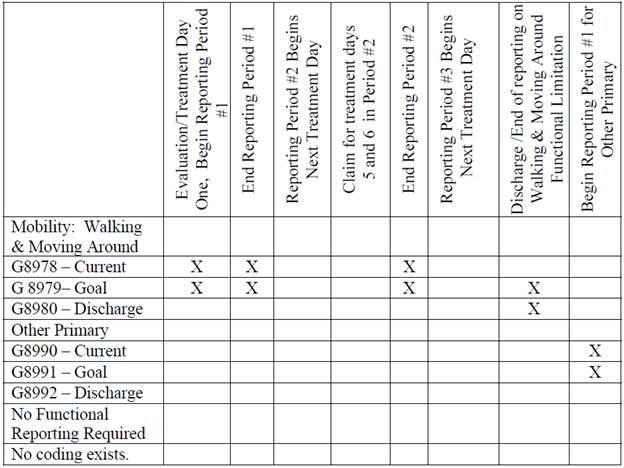
- FLR Reporting Example
What is critical to remember?
There may be a Final Rule published that describes the G-Code in detail, but there is still all the work to be done by the MACs outlining how they will accept and process the claims. There is also an ongoing discussion clarifying what the regulations really mean in all circumstances.
One reason practices partner with Clinicient and invest their time in using our system is to gain efficiency even in the face of more and more documentation burden. When that burden spans the therapist, billing and administrative team, the chances of mistakes, misunderstandings and discrepancies between what is documented and what is reported can put the entire practice at risk. Clinicient eliminates that risk by providing an automated process that prompts the therapist in the normal course of documentation, which will include reporting the severity of functional limitation and converts that into the proper G-Code and modifier. We will alert the therapist and management team until the work is done and we won’t allow claims to be submitted and denied because there isn’t proper reporting on functional outcomes.
If you are interested in learning more about how Clinicient can help your practice reduce it’s risk with these new requirements, we encourage you to learn more.
[NOTE: Medicare does not certify EMR vendors. Some EMR vendors are misleading practices to believe that Medicare has certified their systems for all Medicare requirements. Medicare has never certified EMR systems (otherwise, we’d all be certified!). Some vendors who do not have billing in the same system have had to go the extra step to test their system for PQRS reporting to the Medicare registry since they can not submit via claims. Unfortunately, practices are being mislead to believe EMRs have been “Medicare Certified” giving practices a false sense of security against meeting Medicare requirements, and increasing audit risk.To learn more, click here]


Comments